

The special Oireachtas committee in the Republic of Ireland has just published its final report which recommends that legislation should be introduced to allow for assisted dying. My Death, My Decision welcomes this major development in another jurisdiction neighbouring England and Wales, focusing attention on the lack of progress at Westminster.
Last month the UK Health and Social Care Committee released its own report on assisted dying which, disappointingly, didn’t deliver any recommendation for change.
The Oireachtas committee report made 38 recommendations overall, and outlines that people with incurable, irreversible, progressive and advanced illnesses that will cause death within six months should have access to an assisted death. This time limit should, however be set at 12 months for neurodegenerative conditions.
An important consequence of a law in the Republic is that Irish citizens (or ordinary residents for twelve months) would be eligible. This would allow Northern Irish applicants to be able to access an assisted death in the Republic by virtue of the Irish Nationality and Citizenship Act of 1956 and the Good Friday Agreement.
Trevor Moore, Chair of My Death, My Decision said:
“This Oireachtas committee report on assisted dying takes a welcome, evidence-based and compassionate approach. The proposed narrow time criteria would, however, mean that many people suffering unbearably from incurable conditions like Locked-in Syndrome will be excluded. The politicians will doubtless want to explore this in developing the details.
Politicians in the Northern Ireland Assembly at Stormont may want to move quickly to consider their own assisted dying law, given that their constituents would otherwise have access to assisted dying sooner in the Republic.
Overall, this report follows many others in outlining the overwhelming evidence in favour of assisted dying. Across the British Isles, people are united in wanting change. No-one should have to undergo an unnecessarily painful death when other countries are repeatedly showing that a more compassionate route is possible.”
Notes:
Members of the MDMD team, as well as individuals affected by the current law on assisted dying, are available for interview upon request
For further comment or information, media should contact Nathan Stilwell at nathan.stilwell@mydeath-mydecision.org.uk or phone 07456200033.
My Death, My Decision is a grassroots campaign group that wants the law in England and Wales to allow mentally competent adults who are terminally ill or intolerably suffering from an incurable condition the option of a legal, safe, and compassionate assisted death. With the support of over 3,000 members and supporters, we advocate for an evidence-based law that would balance individual choice alongside robust safeguards and finally give the people of England and Wales choice at the end of their lives.




 The special Oireachtas committee on assisted dying in the Republic of Ireland is set to recommend that legislation should be introduced to allow terminally ill people the right to a dignified death on their own terms. My Death, My Decision welcomes this news, adding to the cases of Scotland, Isle of Man and Jersey in shining a spotlight on the lack of progress at Westminster.
The special Oireachtas committee on assisted dying in the Republic of Ireland is set to recommend that legislation should be introduced to allow terminally ill people the right to a dignified death on their own terms. My Death, My Decision welcomes this news, adding to the cases of Scotland, Isle of Man and Jersey in shining a spotlight on the lack of progress at Westminster.

 Today, the
Today, the 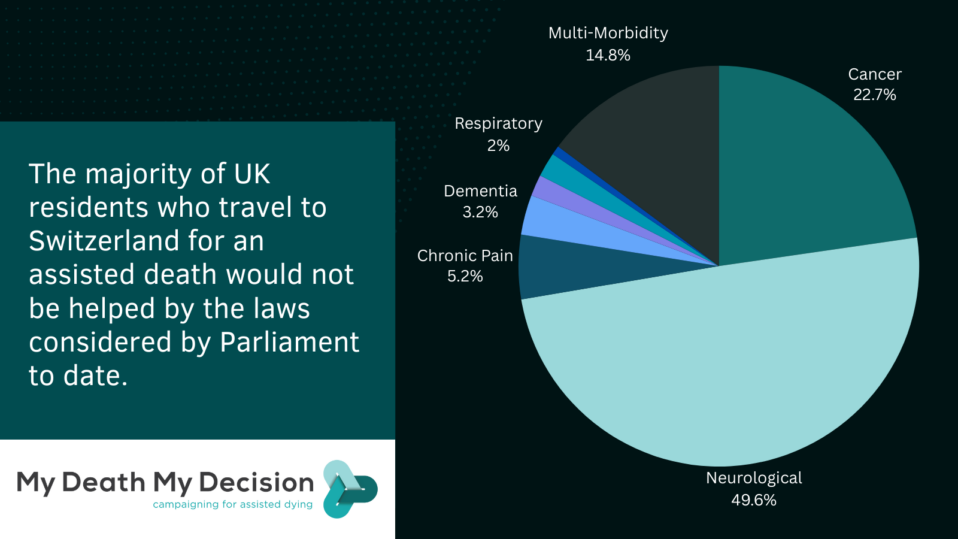
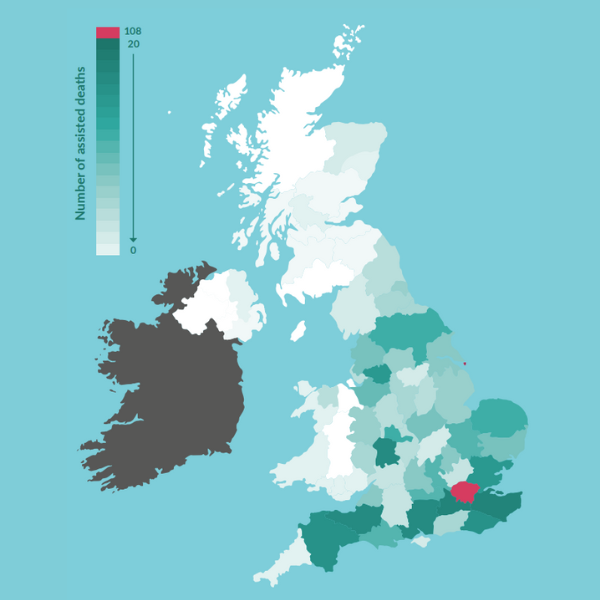
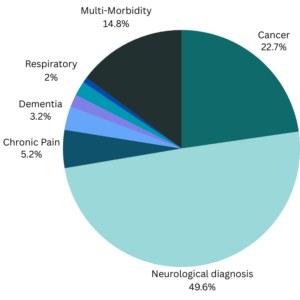 Table 2 UK Residents with neurological diagnoses receiving an assisted death in Switzerland
Table 2 UK Residents with neurological diagnoses receiving an assisted death in Switzerland


 An “ethics review” of assisted dying in Jersey has been published, but campaigners have questioned the need for the review, the scope of the report and the report’s recommendations.
An “ethics review” of assisted dying in Jersey has been published, but campaigners have questioned the need for the review, the scope of the report and the report’s recommendations.

Recent Comments