This should be the last rally this year. I know we’ve asked a lot of you this year, but we need your voice again.
I’m inviting you, and everyone you can bring, to join our rally outside ahead of the next debate in the House of Lords.
Friday 12 September
8:00am to 10:00am
Parliament Square
Why it matters: For any other Bill, the House of Lords normally wouldn’t block it or alter it significantly. The role of the House of Lords is meant to be to tighten laws, making them work better and be more compassionate.
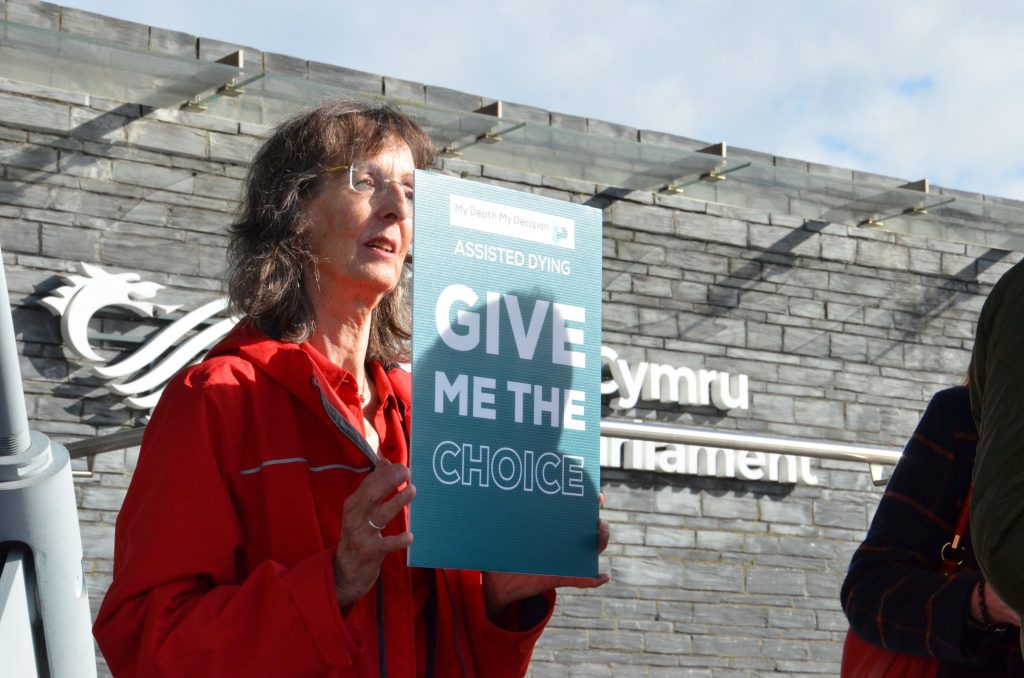
But this is different; some Lords have already said they want to throw the Bill out and stop it in its tracks. We need a strong presence outside parliament to tell them: We want an assisted dying law.
What to expect:
Banners, placards, and posters (feel free to bring your own homemade one!)
Fellow campaigners, including those from Humanists UK
Photography and filming to capture our collective voice
Two of Britain’s most admired actors, Dame Helen Mirren and Pierce Brosnan, have spoken out in support of the right to choose an assisted death.
In a recent interview with Saga Magazine, the stars of The Thursday Murder Club shared their heartfelt views on assisted dying, drawing on personal experiences of seeing loved ones suffer.
Creative Commons Attribution-Share Alike 3.0 Unported license. – Harald Krichel
“I absolutely believe in assisted dying,” said Helen Mirren.
“So do I,” added Pierce Brosnan. “I’ve watched the suffering of dear ones. I think when my time comes, I’d like to be able to have the choice to say: ‘Okay, let’s have that cup of tea and say goodbye.’”
Mirren agreed: “Yes, in a warm and loving way. I do absolutely believe in that.”
Graham Winyard, Director of My Death, My Decision, says:
“It’s powerful to see cultural icons like Helen Mirren and Pierce Brosnan adding their voices to this cause. They reflect what so many families across the UK feel – that compassion, dignity, and choice should guide our laws at the end of life. We want to thank them for their support on this important issue. ”
The Terminally Ill Adults (End of Life) Bill, currently in the House of Lords, would legalise assisted dying for adults with six months left to live or fewer, subject to safeguards and a lengthy process. The next debate in the House of Lords, called Second Reading, will be Friday 12 September.
Notes:
Members of the MDMD team, as well as individuals affected by the current law on assisted dying, are available for interview upon request
For further comment or information, media should contact Nathan Stilwell at nathan.stilwell@mydeath-mydecision.org.uk or phone 07456200033.(media enquiries only)
My Death, My Decision is a grassroots campaign group that wants the law in England and Wales to allow mentally competent adults who are terminally ill or intolerably suffering from an incurable condition the option of a legal, safe, and compassionate assisted death. With the support of over 3,000 members and supporters, we advocate for an evidence-based law that would balance individual choice alongside robust safeguards and finally give the people of England and Wales choice at the end of their lives.
The decision to provide assisted dying through the Welsh NHS will rest with the Senedd, Wales’ Health Secretary has confirmed, though services may still be available privately if the law changes.
Speaking to the Senedd’s Health and Social Care Committee on 16 July, Welsh Health Secretary Jeremy Miles clarified the Welsh Government’s role in implementing the proposed Terminally Ill Adults (End of Life) Bill, which would legalise assisted dying for mentally competent adults with a terminal illness and is currently progressing through Parliament and is due to be debated in the House of Lords on 12 September. If approved, it would become law in England and Wales.
Although the power to enact the Bill rests with Westminster, decisions about service provision in Wales, such as whether NHS Wales can offer assisted dying, fall within devolved health powers. As a result, the Welsh Government would only be able to implement assisted dying through the NHS if the Senedd agrees.
“If the [Welsh] Government wanted to [implement it], and the Senedd didn’t want to approve it – the Senedd would have that ability as well,” Mr Miles said.
Conservative MS Peter Fox, Chair of the Health Committee, sought clarity on whether assisted dying services could be offered through NHS Wales if ministers chose not to lay the necessary regulations.
“If they are not made by the Welsh Government and consequently approved by this Senedd, the NHS in Wales will not be able to provide assisted dying services – is that the case?”
“That is correct,” Mr Miles replied.
He also indicated that decisions about NHS provision would likely be made after the next Senedd election, scheduled for May 2026.
However, the Health Secretary suggested that even without NHS provision, assisted dying could become available in Wales through the private sector, as is the case in other jurisdictions around the world.
This distinction between the legal framework and public service provision has prompted renewed questions about how equitable access will be ensured across the UK.
The former Welsh First Minister, Mark Drakeford, recently raised his own concerns about ensuring assisted dying is accessible in all parts of the UK. Speaking at the Humanists UK convention in Cardiff, he said “I would much rather [assisted dying] was one of those things that we did on a UK-wide basis”. He went on to warn of “the unintended consequences there would be if assisted dying was available in Wrexham but not available in Chester.”
Mark Drakeford talking at the Humanists UK Convention in Cardiff
Graham Winyard, Director of My Death, My Decision, says:
“It would be deeply unjust for people in Wales to be denied access to assisted dying through the NHS while people in England are supported to die on their own terms. Without NHS provision, those who cannot afford private services ,or who are too unwell to travel, may be left without any meaningful choice at the end of life.
Right now, some people are forced to make the traumatic and expensive journey to Switzerland to have the dignified death they deserve. It would be no fairer and no less cruel if people in Wales were forced to travel across the border to England instead.
We hope that whoever is in Government in Wales after the May election will ensure that everyone facing a terminal illness, regardless of where they live or what they earn, is treated with the compassion, dignity, and respect they deserve.”
Before the election, Members of the Senedd will have a say on a Legislative Consent Motion (LCM), a formal vote used when Westminster legislates on devolved matters. Although not legally binding, such motions carry significant political weight under the Sewel Convention, which states that the UK Parliament will “not normally” legislate on devolved matters without consent.
Mr Miles confirmed that the outcome of this vote would influence the Welsh Government’s next steps.
The Senedd has previously voted against the principle of assisted dying — most recently in 2023, by 26 votes to 19, with 9 abstentions. A similar motion was rejected in 2014. However, the current Bill is more narrowly drawn, applying only to mentally competent adults with a terminal illness, and includes a clear legal framework and strict safeguards.
Notes:
Members of the MDMD team, as well as individuals affected by the current law on assisted dying, are available for interview upon request
For further comment or information, media should contact Nathan Stilwell at nathan.stilwell@mydeath-mydecision.org.uk or phone 07456200033.
My Death, My Decision is a grassroots campaign group that wants the law in England and Wales to allow mentally competent adults who are terminally ill or intolerably suffering from an incurable condition the option of a legal, safe, and compassionate assisted death. With the support of over 3,000 members and supporters, we advocate for an evidence-based law that would balance individual choice alongside robust safeguards and finally give the people of England and Wales choice at the end of their lives.
[The deadline to apply for board positions is 21 September]
My Death, My Decision is a grassroots movement that campaigns for assisted dying reform. We want a compassionate law on assisted dying that permits a medically assisted death to adults of sound mind who are suffering intolerably or terminally ill. We believe reform is necessary to reduce the suffering of individuals who are close to death, and, just as importantly, to give choice to those with physical, incurable conditions who face years of constant pain or suffering that they find unbearable.
My Death, My Decision has been at the forefront of supporting the Terminally Ill Adults (End of Life) Bill while recognising that it does not fulfill all our goals. It has become increasingly clear that a long-term campaign will be necessary after the Bill is passed, both to ensure that the Bill is properly implemented and to engage with future reviews and consultations.
We are seeking expressions of interest now so that we are well-placed to manage this change effectively.
What are we looking for?
We are looking for people who share our passion for what should be a basic human right and are interested in active hands-on involvement in the campaign. In particular, we would like to attract people with the following experience and expertise:
Chairing a charity or managing a small organisation.
Public Affairs or Campaigning
Medicine
Fundraising or Marketing
Policy or Legal
Operations
We are an equal opportunities employer, proud of our diversity and Board gender balance. We remain committed to improving our diversity and therefore encourage applications from all members of the community.
Experience in charity governance would be welcome.
What will you be doing?
My Death, My Decision is a small grassroots organisation. Many people are often surprised to see how much work is carried out by so few staff members and that we are volunteer-led.
We are looking to recruit a working board, more than a governing board, meaning that the board will be expected to fulfil a hands-on volunteering role, with clear tasks and responsibilities, rather than the boards of larger organisations, which generally only advise and set the strategy.
The time commitment will be between 2 to 4 hours per week, depending on your expertise and what tasks you volunteer to support with.
What difference will you make?
This is an opportunity to effect real change and make a difference by achieving law change that will respect autonomy, ensure dignity and end unnecessary suffering for those at the most challenging times of their lives; and provide choice for those making critical decisions about their lives and how they might end.
We are committed to an evidence-based law which balances individual choice alongside robust safeguards. You can be the dynamic motivator of the work of our members, supporters, patrons and activists as we help to enshrine the values of autonomy, dignity, and compassion into assisted dying legislation.
Next steps:
If you are interested in playing a role in one of the biggest campaigns in a generation please send a CV and a short introduction email explaining why you would like to join the board and what expertise you will bring to our grassroots organisation.
As you can imagine, we are in the busiest period our campaign has ever seen. We will endeavour to acknowledge receipt of all applications and will seek to host interviews on a rolling basis.
Please send applications to: simon.menneer@mydeath-mydecision.org.uk with the subject line: “Board Recruitment”.
[The deadline to apply for board positions is 21 September]
The Terminally Ill Adults (End of Life) Bill has passed Third Reading in the House of Commons. The vote was 314 in favour, 291 against. My Death, My Decision and Humanists UK welcome the result.
Carmen Sumadiwiria, Director of Diversity at My Death, My Decision said:
‘This is a day for the history books, where facts have prevailed over fear. Today’s vote reflects what the British public has known for years, that everyone deserves the right to choose a compassionate death. We are grateful to politicians who listened to evidence, reason, and the lived experience of dying Brits. This is a momentous victory for the overwhelming majority who support assisted dying, and we will keep working to make sure those voices continue to be heard.
‘We want to thank every parliamentarian who stood up today for dignity and common sense. Your courage has given hope to terminally ill adults across the country who simply want the choice to die peacefully and on their own terms. We are proud to stand with you and will continue to work for a fairer, kinder law.’
Andrew Copson, Chief Executive of Humanists UK, said:
‘The House of Commons has taken a historic step towards meeting the aspirations of the public, who overwhelmingly support having choice, dignity, and compassion at the end of their lives. We welcome this and now look forward to working with Lords on the legislation.
‘MPs have finally recognised the fact that assisted dying is already happening in this country. People are travelling to Switzerland if they have the money and mobility to do so. Others are dying in traumatic circumstances by suicide. Many more are suffering greatly, even while receiving the best possible care. Today, we are a significant step closer to ending that unnecessary and cruel suffering and MPs should be commended for taking this step. ’
Louise Shackleton accompanied her husband, Anthony, to Switzerland for an assisted death after he had been suffering from motor neurone disease for six years. She said:
‘Today, the majority of MPs did the right thing. They listened with compassion, and they chose dignity over fear. I’m so relieved that other families won’t have to go through what Anthony and I did, forced to leave our home, our loved ones, and our country just so he could have a peaceful death.
‘This law means that people facing unimaginable illnesses will finally have a choice. It means their final days can be filled with love, not fear, with family, not police interviews. I promised Anthony I’d fight for this, and today I can say we’ve been heard.’
The Bill will now progress to the House of Lords, which will further scrutinise it. It applies to England and Wales only. A private member’s bill in Scotland by Liam McArthur MSP recently passed its First Stage vote in the Scottish Parliament.
Notes
For further comment or information, media should contact Humanists UK Director of Public Affairs and Policy Richy Thompson at press@humanists.uk or phone 0203 675 0959 or My Death My Decision Director of Diversity Carmen Sumadiwiria at carmen.sumadiwiria@mydeath-mydecision.org.uk or phone 07879 391313
Humanists UK and My Death, My Decision have people and their loved ones who would be affected by this change available for the press. If you have been affected by the current assisted dying legislation, and want to use your story to support a change in the law, please email campaigns@humanists.uk.
Humanists defend the right of each individual to live by their own personal values, and the freedom to make decisions about their own life so long as this does not result in harm to others. Humanists do not share the attitudes to death and dying held by some religious believers, in particular that the manner and time of death are for a deity to decide, and that interference in the course of nature is unacceptable. We firmly uphold the right to life but we recognise that this right carries with it the right of each individual to make their own judgement about whether their life should be prolonged in the face of pointless suffering.
We recognise that any assisted dying law must contain strong safeguards and the international evidence from countries where assisted dying is legal shows that safeguards can be effective. We also believe that the choice of assisted dying should not be considered an alternative to palliative care, but should be offered together as in many other countries.
Humanists UK is the national charity working on behalf of non-religious people. Powered by over 130,000 members and supporters, we advance free thinking and promote humanism to create a tolerant society where rational thinking and kindness prevail. We provide ceremonies, pastoral care, education, and support services benefitting over a million people every year and our campaigns advance humanist thinking on ethical issues, human rights, and equal treatment for all.
My Death, My Decision is a grassroots campaign group that wants the law in England and Wales to allow mentally competent adults who are terminally ill or intolerably suffering from an incurable condition the option of a legal, safe, and compassionate assisted death. With the support of over 3,000 members and supporters, we advocate for an evidence-based law that would balance individual choice alongside robust safeguards and finally give the people of England and Wales choice at the end of their lives.
Humanists UK and My Death, My Decision are both members of the Assisted Dying Coalition, along with Friends at the End, Humanist Society Scotland, and End of Life Choices Jersey.
On Friday 20 June, politicians will debate further changes to the Bill, and vote on the Bill as a whole. This means the Bill could pass on to the next stage, or fail entirely.
Today MPs debated the Terminally Ill Adults (End of Life) Bill as part of Report Stage. They debated a series of amendments, and voted on two.
The changes to the Bill debated today were: ‘Obligations, duties and protections for medical practitioners, hospices and care homes; The procedure for receiving assistance under the Act including safeguards and protections; Eligibility and mental capacity.’
Amendment NC10 (widening opt-outs) was agreed to without a vote. Amendment (a) to NC10, which would essentially have allowed employers as a whole to opt their employees out regardless of the employees’ views, was defeated 279 to 243.
Claire Macdonald, Director of My Death, My Decision, said:
“Today’s debate shows just how important it is that we give people real choice and control at the end of their lives. No one should be forced to suffer against their will when they’re dying. We support this Bill because it’s about kindness, dignity, and making sure the law reflects the compassion most people already feel.”
MPs will return on 13 June to debate amendments on: ‘Approved substances and devices; Advertising; Inquests; investigations and death certification; Guidance and codes of practice; Welsh language; Monitoring, consultation and reviews; The Assisted Dying Commissioner; Implementation; Regulations; Extent; Commencement.’ Following this debate, they will vote on chosen amendments – including those from today that were not yet voted upon. It is unclear as to whether they will get through all votes on 13 June. If not, they will continue onto 20 June. After that, they will have Third Reading, where they will vote on the Bill again as a whole.
Notes
Members of the MDMD team, as well as individuals affected by the current law on assisted dying, are available for interview upon request
For further comment or information, media should contact Nathan Stilwell at nathan.stilwell@mydeath-mydecision.org.uk or phone 07456200033 (media only).
My Death, My Decision is a grassroots campaign group that wants the law in England and Wales to allow mentally competent adults who are terminally ill or intolerably suffering from an incurable condition the option of a legal, safe, and compassionate assisted death. With the support of over 3,000 members and supporters, we advocate for an evidence-based law that would balance individual choice alongside robust safeguards and finally give the people of England and Wales choice at the end of their lives.
The Scottish Parliament has voted in favour of the Assisted Dying for Terminally Ill Adults (Scotland) Bill. Members of the Assisted Dying Coalition have welcomed the vote.
MSPs voted 70 in favour, 56 against on Stage 1 of the Bill, which is about general principles. There will be another two rounds of voting and amendments before the Bill passes fully. No Assisted Dying Bill in Scotland has ever made it past Stage 1.
Emma Cooper, Convenor of Friends at the End, said:
‘Today is a landmark moment for compassion, dignity, and choice in Scotland. As someone who has seen firsthand the pain that can accompany the end of life, I know how vital it is that we give people the right to die on their own terms. This Bill is not about giving up, it’s about empowering those who are dying to have control, peace, and a say in their final days. While this is not yet law, passing Stage 1 means the Scottish Parliament now has the opportunity to consider amendments and work together to create the right legislation for Scotland. On behalf of Friends at the End, we welcome this historic step forward and stand with all those who have waited so long for this moment.’
Claire Macdonald, Director of My Death, My Decision, said:
‘Today’s decision is a monumental step forward for human rights and compassion. This victory demonstrates Scotland’s leadership in recognising the fundamental right of terminally ill individuals to make dignified and autonomous choices about their own deaths. No-one should be forced to suffer at the end of life, and this law ensures that terminally ill adults will now have greater control and peace of mind.’
Glasgow-based Kevan Donoghue died at age 64, 18 months after a shock diagnosis of a rare bile duct cancer. Suffering from constant pain, Kevin died after not eating or drinking for three weeks as a result of his illness. His wife, ex-nurse Patricia Donoghue, suffers from PTSD following her husband’s death. Commenting on the vote, Patricia Donoghue said:
‘I am relieved and pleased with this result. It is a significant step forward for supporters of this legislation. It won’t immediately change the law, but it indicates real backing in the Scottish Parliament to continue refining and debating the Bill. It is a major milestone as previous attempts in Scotland have failed. Scotland is moving towards legally assisted dying for terminally ill adults. The hard work continues.’
Introduced by Liberal Democrat MSP Liam McArthur, the Assisted Dying for Terminally Ill Adults (Scotland) Bill is a Private Member’s Bill. It will allow terminally ill adults in Scotland to lawfully request, and be provided with, assistance by health professionals to end their own life.
Westminster will debate amendments to the Terminally Ill Adults (End of Life) Bill, which will apply to England and Wales, at Report Stage on Friday 16 May. Assisted dying legislation in the Isle of Man passed in March and is awaiting royal assent.
Humanists UK, My Death, My Decision, Humanist Society Scotland, and Friends at the End are all part of the Assisted Dying Coalition, a group of organisations across the UK and Crown Dependencies who campaign for a compassionate assisted dying law
Notes:
Members of the MDMD team, as well as individuals affected by the current law on assisted dying, are available for interview upon request
For further comment or information, media should contact Nathan Stilwell at nathan.stilwell@mydeath-mydecision.org.uk or phone 07456200033 (media only).
My Death, My Decision is a grassroots campaign group that wants the law in England and Wales to allow mentally competent adults who are terminally ill or intolerably suffering from an incurable condition the option of a legal, safe, and compassionate assisted death. With the support of over 3,000 members and supporters, we advocate for an evidence-based law that would balance individual choice alongside robust safeguards and finally give the people of England and Wales choice at the end of their lives.
The Government’s impact assessments for the Terminally Ill Adults (End of Life) Bill, published today, demonstrate that assisted dying can be delivered safely, ethically, and compassionately in England and Wales. Humanists UK and My Death, My Decision have welcomed the reports.
Coming two weeks before the Bill returns to the Commons for the next stage of legislative scrutiny, the impact reports outline the costs associated with the law and the impact on different groups, drawing from evidence in 25 other jurisdictions where assisted dying is already established.
Overall there are predicted to be cost savings for the state if the law does change – though the sums of at most tens of millions are negligible in the context of the £180 billion annual NHS spend. Regardless, the decision on whether to change the law should not be about economics, but on whether assisted dying is the right approach in principle.
Terminally ill people of sound mind who have a clear and settled wish to die are suffering enormously under the law as it stands, or else finding ways to end their lives without safeguards. This Bill will enable them to end their lives with appropriate safeguards through a proper legal framework.
Pictured: left to right Dr Emma Boulton, Kim Leadbeater MP, Rachel Hopkins MP, Lizzi Collinge MP – Humanists UK and My Death, My Decision parliamentary reception
Andrew Copson, Chief Executive of Humanists UK said:
‘These impact assessments are part and parcel of the scrutiny process that effective legislation requires, adding another layer to a Bill that has already seen months of thorough debate in the House of Commons at committee stage in addition to its pre-legislative development. We’re pleased to see that the Government has done such a thorough job.
‘Assisted dying isn’t untested. Legislation is already working in over 31 jurisdictions across the world, where implementation in Australia, New Zealand, the US, and Europe has shown it to be safe, compassionate, and practical. It’s time for Parliament to grant people the dignity and autonomy they deserve at the end of life.’
Claire Macdonald, Director of My Death, My Decision said:
‘These reports confirm what we have long known – that our current laws are failing dying people and that the current status quo is unacceptable. Every day we delay is another day someone is denied the choice to die with dignity, free from prolonged pain and suffering.
Assisted dying is not a fringe issue – it is a mainstream, compassionate cause backed by the majority of the public. These reports must be a catalyst for action. It’s time for Parliament to take a clear-eyed, humane look at how we care for those at the end of their lives.’
On 16 May, all MPs will have the opportunity to debate the Bill for the first time since it was strengthened considerably by its public bill committee. The impact assessments’ findings have shown that the Bill is feasible and workable, as well as overwhelmingly supported by UK citizens.
In March, the Isle of Man became the first jurisdiction in the UK and Crown dependencies to pass an assisted dying law following a historic vote. The Bill will make assisted dying available to adult Isle of Man residents who are of sound mind, are terminally ill, have twelve months or fewer to live, and have a clear and settled wish to die.
Notes:
Members of the MDMD team, as well as individuals affected by the current law on assisted dying, are available for interview upon request
For further comment or information, media should contact Nathan Stilwell at nathan.stilwell@mydeath-mydecision.org.uk or phone 07456200033.
My Death, My Decision is a grassroots campaign group that wants the law in England and Wales to allow mentally competent adults who are terminally ill or intolerably suffering from an incurable condition the option of a legal, safe, and compassionate assisted death. With the support of over 3,000 members and supporters, we advocate for an evidence-based law that would balance individual choice alongside robust safeguards and finally give the people of England and Wales choice at the end of their lives.
Here’s everything you need to know about these assessments.
What do the Impact Assessments focus on?
The extensive impact assessments focus a lot on analysis of the financial implications of the Bill. However, the Government recognises that doesn’t truly reflect the impacts the Bill will have, saying: ‘adding only the quantified elements of [the impact assessment] together would not give a comprehensive assessment on the net impact of the Bill because significant unquantified impacts would not be accounted for in that net figure’.
In other words, it does not take into account the human costs of doing nothing. We have produced a separate report on this, which highlights that:
Thousands of terminally ill adults would continue to suffer every year if the Bill is not passed, with many forced to take their own lives, even with the best possible standard of palliative care
Legalising assisted dying is linked to an increase in the provision of palliative care,alongside bringing peace of mind to individuals who choose to avail of an assisted death
The current situation exports compassion abroad, creating inequalities based on wealth, resources, and family support
A broken system subjects families to harsh, intrusive investigations for acts of compassion, which are very rarely prosecutable.
Safeguards and Protections
The Bill includes strong protections to ensure people are eligible, informed, and choosing freely.
Key features:
Two independent doctors must agree the applicant qualifies.
A panel (doctor, psychiatrist, social worker) reviews each case.
Mandatory reflection periods to allow reconsideration.
Disability Advisory Board and advocates involved.
Mandatory training on recognising coercion, and supporting disabled and autistic people.
As the Impact Assessment confirms:
‘The Bill goes further than some other jurisdictions in terms of oversight, regulation, protections and safeguards.’
Professional Autonomy
The Impact Assessment confirms again that healthcare professionals can opt out if they object – no one is forced to participate.
Fair Access for All
The assessments recognise concerns about how the Bill might impact disabled people. To address this, the Bill includes specific safeguards to protect against pressure or coercion and to ensure decisions are truly voluntary.
These measures are designed to protect, not exclude, disabled people;ensuring safety, autonomy, and equal dignity for all who are eligible.
The Government’s analysis also confirms that the new law will also offer compassion to people who cannot afford to travel abroad for assisted dying.
Financial Considerations
Although the Bill is driven by compassion, not cost-saving, the Government’s assessments show it is also affordable:
Healthcare savings: Less end-of-life care for people who choose an assisted death could save the NHS up to £59.6m per year by year 10.
Implementation costs (oversight panels, training, admin): estimated to be £13.5–25.1m per year by year 10 – which would be covered by healthcare savings.
Training: To ensure safe, informed care – up to £11.4 million in year 1 for initial training, then up to £9.7 million annually by year 10.
Benefits and pensions: Fewer pension and benefits payments needed for those choosing an assisted death – up to £27.7 million annually saved by year 10.
Court and admin costs: Minimal and manageable within current capacity.
Overall: The impact assessments show this is a compassionate policy that doesn’t strain public resources.
International Context
The Terminally Ill Adults Bill’s approach reflects best practices from countries like:
Australia
New Zealand
Oregon (USA)
These systems show that assisted dying can be implemented safely and fairly.
Human Rights Compliance
The Government has confirmed the Bill is compatible with human rights law, aligning with the . It upholds:
The right to life
The right to dignity and autonomy
Protection from suffering
In Summary
According to the Government’s own analysis, the Bill is:
Morally justified
Affordable
Safe
Practically deliverable
A compassionate law that gives terminally ill adults the dignity of choice.
The Terminally Ill Adults (End of Life) Bill is a landmark piece of legislation and an opportunity to extend freedom of choice and dignity at the end of life for thousands of Britons.
The Impact Assessment is part and parcel of the scrutiny process that good legislation requires – adding another layer to a Bill that has already seen months of expert testimonial, thorough, and over 90 hours of thoughtful debate by colleagues across the House at Committee Stage.
Report Stage is due to take place on Friday 16 May although could run to Friday 13 June; and Third Reading is likely scheduled for Friday 13 June, although could be Friday 20 June if Report Stage overruns.









 Before the election, Members of the Senedd will have a say on a Legislative Consent Motion (LCM), a formal vote used when Westminster legislates on devolved matters. Although not legally binding, such motions carry significant political weight under the Sewel Convention, which states that the UK Parliament will “not normally” legislate on devolved matters without consent.
Before the election, Members of the Senedd will have a say on a Legislative Consent Motion (LCM), a formal vote used when Westminster legislates on devolved matters. Although not legally binding, such motions carry significant political weight under the Sewel Convention, which states that the UK Parliament will “not normally” legislate on devolved matters without consent.

 My Death, My Decision is a small grassroots organisation. Many people are often surprised to see how much work is carried out by so few staff members and that we are volunteer-led.
My Death, My Decision is a small grassroots organisation. Many people are often surprised to see how much work is carried out by so few staff members and that we are volunteer-led.





 Today MPs debated the Terminally Ill Adults (End of Life) Bill as part of Report Stage. They debated a series of amendments, and voted on two.
Today MPs debated the Terminally Ill Adults (End of Life) Bill as part of Report Stage. They debated a series of amendments, and voted on two.
 The Scottish Parliament has voted in favour of the Assisted Dying for Terminally Ill Adults (Scotland) Bill. Members of the Assisted Dying Coalition have welcomed the vote.
The Scottish Parliament has voted in favour of the Assisted Dying for Terminally Ill Adults (Scotland) Bill. Members of the Assisted Dying Coalition have welcomed the vote. Emma Cooper, Convenor of Friends at the End, said:
Emma Cooper, Convenor of Friends at the End, said: Glasgow-based Kevan Donoghue died at age 64, 18 months after a shock diagnosis of a rare bile duct cancer. Suffering from constant pain, Kevin died after not eating or drinking for three weeks as a result of his illness. His wife, ex-nurse Patricia Donoghue, suffers from PTSD following her husband’s death.
Glasgow-based Kevan Donoghue died at age 64, 18 months after a shock diagnosis of a rare bile duct cancer. Suffering from constant pain, Kevin died after not eating or drinking for three weeks as a result of his illness. His wife, ex-nurse Patricia Donoghue, suffers from PTSD following her husband’s death. 

 What’s this about?
What’s this about?


Recent Comments